After a year of basically being out of business due to various forms of lockdown, I have returned from thinking about respiratory disease pandemics to thinking about the other pandemic. The one that started about 50 years ago, got worse and worse for each of those 50 years and has claimed countless lives. Countless, mainly because nobody has bothered to count them. It’s also now suspected of making the disease of the pandemic of the last two years even worse than it would otherwise be. Obesity.
I’ve written many times about my view. The obesity pandemic has been caused by the replacement in the human diet of fat by sugar and highly processed carbohydrates. I’ve formed this view based on my own experience of being obese for many years and trying and failing to lose weight by restricting calorie intake principally by severely restricting fat in my diet (the Energy Balance Model) and the sudden, rapid, and sustained weight loss I experienced when I severely restricted carbohydrates in my diet (the Carbohydrate-Insulin Model). Also, I would note that, when I severely restricted fat in my diet I felt terrible, but when I severely restricted carbohydrates I felt better than ever.
At this point I can hear a few people wandering off shaking their heads and saying, “Well if he’s going to restrict something “severely” then he deserves to feel terrible!”. To which I say, you can’t make a big change without making a BIG CHANGE. Plus eliminating carbs made me feel better not worse!
I would just like to be clear that no one told me that restricting carbohydrates would cause me to lose weight. I hadn’t read a book about it or taken advice from a guru or scoured scientific journals, it was a matter of simple observation, over dinner in a restaurant in Paris in 2003. Every woman in the restaurant was thin and not one of them (that I could see) had any carbohydrates of any description on her plate. The women were mostly eating steak and green salad with an olive oil dressing. So, I decided to try what I thought they were doing and miraculously started to lose weight. It was only when, during a routine check-up, I told the practice nurse at my doctor what I was doing, she told me about the famous Dr Atkins. I had never heard of him until then.
Since then, I have, of course, read the esteemed Doctor’s books, discovered William Banting, John Yudkin, Thomas Cleave, Mark Sissons, Nina Teicholz, Gary Taubes and many others who, in general, all seem to hold the same view that I had come to – that it was carbohydrate intake that drives weight gain and not fat intake. The thing that links all these writers together is that they try to describe the mechanism by which it would be possible for carbohydrate intake to drive weight gain by causing excess insulin secretion which increases the deposition of fat in the adipose tissue of the body. The Carbohydrate-Insulin Model (CIM).
Below is the CIM as a diagram. The numbered arrows in the diagram indicate a scientifically testable hypothesis that is considered in the peer reviewed paper I refer to later.
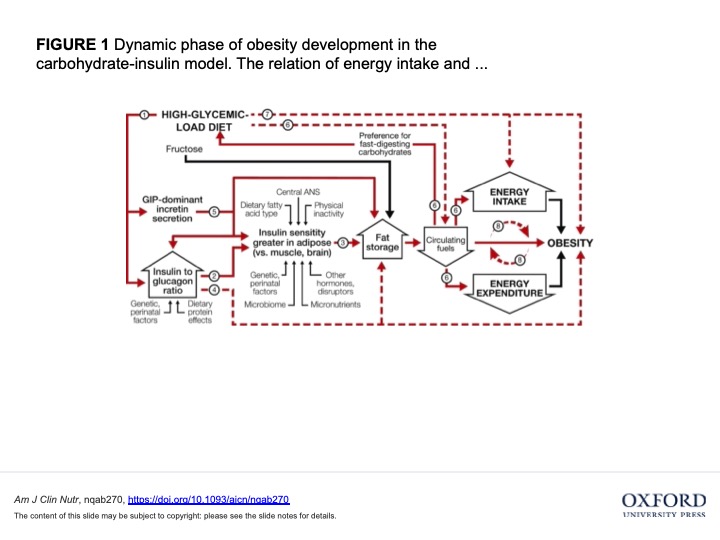
Ludwig et al American Journal of Clinical Nutrition
However, for more than 50 years we have been told by the large majority of the medical and scientific establishment that it is the Energy Balance Model (EBM) that was the correct model, and that the obesity pandemic was caused by people simply eating more calories than they needed for the amount of physical activity they were doing. This seems strange to me as, as far as I am aware, people are now eating FEWER calories than they were 50 years ago and still getting fatter. So I am puzzled as to where the evidence is to support this EBM model or what the mechanism would be that would drive it. In my experience, people that advocate the EBM do not try to describe any mechanism by which the overconsumption of calories of itself causes the body to lay down more fat than it otherwise would do rather than, say, raise your basal metabolic rate to burn off this excess energy to preserve your body weight set point. As homeostasis would suggest it would. The human body does not like change. They just say things like “move more, eat less” or “it’s obvious that if you eat more than you need to for the exercise you do, you will get fat”. I have many problems with these statements but in particular;
a) If you move more, you will probably eat more and if you eat less you will probably move less; and
b) Can you point me to the evidence which shows that if you eat more calories than you need, you will get fat simply because of those additional calories? Or are you just fat shaming people as greedy and lazy, when they are actually suffering from a serious disease?
Which may sound a bit grumpy but having been the recipient of this EBM advice which drove me to severely restrict fat in my diet that made me feel terrible, I feel I have the right! This advice also requires you to swallow two other unproven assumptions
a) that all calories have the same effect on the body – a calorie is just a calorie, no matter what food it comes from; and
b) If a) is true, the best was to reduce calorie intake is to cut fat from your diet as it has the most calories per gram.
The problem with a) is that it simply isn’t true. Different foods have very different effects on insulin production which, among other things, promotes fat storage. The problem with b) is that your body needs dietary fat for many vital functions of the body, and I mean MANY. Therefore, if you don’t eat enough of it, you will feel TERRIBLE. What your body does not need is dietary carbohydrates. If your body needs some glucose, it will simply make what it needs. You do not need to eat any carbs at all, and if you don’t eat any, you will feel FINE.
So far, so much my view of the world and an unreferenced one at that! It would be a reasonable question to ask where my evidence is for the all the above. Well, I deliberately didn’t reference anything as I no longer have to! Quite a lot of high powered doctors, scientists and journalists (including the ever-present Gary Taubes) have done it for me in a peer reviewed paper in the American Journal of Clinical Nutrition:
https://academic.oup.com/ajcn/advance-article/doi/10.1093/ajcn/nqab270/6369073?searchresult=1
For me, while the whole paper is well worth reading, the standout argument for change is contained in this paragraph:
Furthermore, conceptual adoption of the EBM has failed to stem the obesity pandemic. Governments and professional health organizations heavily promote energy restriction (especially with low-fat diets) and exercise; nutrition labels on packaged foods prominently display calorie content; and personal responsibility to avoid excess weight gain is emphasized in patient care. Nevertheless, obesity prevalence continues to increase worldwide, prompting spectacularly complex formulations of the EBM addressing myriad biological, behavioural, environmental, and societal factors converging on energy balance, with questionable practical translation.
In other words, you establishment types have been running this unethical EBM experiment for 50 years. You now have a lot of results across the world to look at and they all say the same thing – EBM as a means of controlling the obesity pandemic DOES NOT WORK.
If the thought of reading a scientific paper isn’t your thing, never fear! In one of those coincidences that are hard to explain, in today’s Observer newspaper there is an article which makes many of the same points in an easy-to-read form:
The authors also make the point that nothing of what they are saying is new and can track back the CIM to almost a century ago (see the table below). I think they could have gone quite a lot further than that. William Banting (c. December 1796 – 16 March 1878) was a notable English undertaker. Formerly obese, he is also known for being the first to popularise a weight loss diet based on limiting the intake of carbohydrates, especially those of a starchy or sugary nature in 1863!!
Some people heeded Mr Banting’s advice and still do – in South Africa there are restaurants that describe themselves as “Banting Friendy”! That’s quite an impressive legacy to leave behind you.
TABLE 1
Historical precedents regarding the carbohydrate-insulin model of obesity
| Year | Authors | Quotation |
| 1924 | Harris (164) | “[O]ne of the causes of hyperinsulinism is the excessive ingestion of glucose-forming foods … It is possible that the hunger incident to hyperinsulinism may be a cause of overeating, and, therefore, the obesity that so often precedes diabetes.” |
| 1938 | Wilder and Wilbur (165) | “[It seems that] mobilization of fat from fat depots is resisted in obesity and that deposition is accelerated…. The effect after meals of withdrawing from the circulation even a little more fat than usual might well account both for the delayed sense of satiety and for the frequently abnormal taste for carbohydrate encountered in obese persons. Energy requirements must be satisfied one way or another, and if part of the food is made less available for metabolism, the result, as is the case in diabetes, inevitably is hunger. A slight tendency in this direction would have a profound effect in the course of time.” |
| 1941 | Bauer (166) | “The current energy theory of obesity, which considers only an imbalance between intake of food and expenditure of energy, is unsatisfactory…. An increased appetite with a subsequent imbalance between intake and output of energy is the consequence of the abnormal anlage [predisposition] rather than the cause of obesity.” |
| 1942 | Hetherington and Ranson (42) | “[High calorie intake and a sedentary life] may be only symptomatic, and not fundamental. It is not difficult to imagine, for example, a condition of hidden cellular semistarvation caused by a lack of easily utilizable energy-producing material, which would soon tend to force the body either to increase its general food intake, or to cut down its energy expenditure, or both.” |
| 1953 | Pennington (167) | “[Caloric restriction] reduces the weight of anyone, obese or lean, regardless of metabolic status, by opposing the homeostatic mechanism for maintaining energy balance. A more rational form of treatment, then, would be one which would enable the organism to establish a homeostatic equilibrium between caloric intake and expenditure at a normal level of body weight. In such a case, treatment would be directed primarily toward mobilization of the adipose deposits, and the appetite would be allowed to regulate the intake of food needed…. The use of a diet allowing an ad libitum intake of protein and fat and restricting only carbohydrate appears to meet the qualifications of such a treatment.” |
| 1957 | Thorpe (168) | “Restriction of carbohydrate intake removes the stimulus to insulin production, so that the fat storage activity of insulin will be held to a minimum. … Fat will be mobilized from the adipose deposits of the body, oxidized to ketones in the liver, and circulated to the tissues in this easily combustible form…. [F]or it has long been known that, while carbohydrate can be readily converted into fat in the body, fat cannot be converted into carbohydrate in any significant amounts.” |
| 1965 | Berson and Yalow (169) | “The precise relationship of obesity to diabetes is not clear. We generally accept that obesity predisposes to diabetes; but does not mild diabetes predispose to obesity? Since insulin is a most potent lipogenic agent, chronic hyperinsulinism would favor the accumulation of body fat.” |
